
Factors influencing coverage of HIV pre-exposure prophylaxis (PrEP) in Australia
By Dean Murphy
Background
Australia is considered to be a leading country in the provision of PrEP to populations at risk of HIV infection. The current national HIV strategy includes an aim of increasing to 75% the proportion of eligible people who are on PrEP. AFAO’s recent policy statement, Agenda 2025: Ending HIV Transmission in Australia, has called for 95% of people for whom PrEP is beneficial to be using it by 2025 [1].
Drawing on peer-reviewed literature, health promotion and policy documents, and interviews with key informants in Australia (supplemented by comparative interviews with informants from other countries), this essay analyses current and historical factors influencing PrEP access and uptake in Australia.
Between June 2014 – when the first PrEP demonstration project commenced [2] – and April 2018 – when PrEP became widely available through listing on the Pharmaceutical Benefits Scheme (PBS) – over 14,000 people accessed PrEP through studies and then general prescribing [2-5]. Despite their relatively modest size, these studies – specifically the larger studies conducted between 2016 and 2018 – contributed to a decline in HIV notifications in men who have sex with men (MSM) during this period. For example, the EPIC study (fig. 1), which commenced in 2016 in New South Wales [6], reported a 25.1% reduction in new HIV infections in gay and bisexual men during the 12 months following the study’s commencement and a 18.5% reduction in other HIV diagnoses [7]. The equivalent Victorian study, PrEPX [8] (fig. 2), contributed to a 30% decline in new HIV infections in men reporting sex with other men in the three years after the study started, compared to the three years prior to the study. In addition, there was a 16% decline in total HIV infections among this group following the commencement of the study [9].
However, other populations at risk of HIV infection have not experienced a decline in HIV infections, over the same period. In Australia overall there has also been a mixed picture in relation to HIV notifications. In 2019, there was a decline of 12 per cent over the previous five years, although a slight increase from the year before [10]. Among gay and bisexual men, HIV diagnoses have declined by over 20% in the past five years. The number of new HIV diagnoses among Indigenous Australians fluctuated over the last five years, but Aboriginal and Torres Strait Islander peoples continue to be diagnosed with HIV at a higher rate than Australian-born non-Indigenous Australians. In 2016 HIV notification rates in Indigenous Australians were 2.2 times higher than in Australian born non-indigenous population’ [11]. The numbers of new HIV diagnoses among heterosexuals and people born overseas have remained steady since 2015, and there has been a slight increase among people who inject drugs.
Even among gay and bisexual men, despite an overall decline in HIV diagnoses, this decline has not been consistent across all sub-groups. Although HIV diagnoses have decreased among Australian-born men, they have increased among overseas-born men, and among men who inject drugs. Even prior to the broader availability of PrEP (via the PBS), differing patterns in HIV diagnosis rates were emerging in infections attributed to male-to-male sex, with national data showing increases in diagnoses among men born in Asia and the Americas [12]. Analyses of infections at Melbourne’s major sexual health centre (which accounts for around one-third of all new diagnoses in Victoria) found that incident HIV infections fell in Australian-born men but did not fall in recently arrived Asian-born men [13].
PrEP use
There is need for more research to identify the reasons why some people who are ‘eligible’ for PrEP have not taken it up. However, some information is available regarding the socio-demographic factors associated with non-uptake in Australia and elsewhere, for example younger age, cultural-ethnic background, and being less socially engaged with gay men [15-20]. Also, a range of attitudinal and social/relational factors have been identified – such as concerns about side effects, perceived (and/or actual) risk of HIV [21-23], being more socially engaged with gay men and other PrEP users [15-19, 24], and specifically among African migrants, stigma and health literacy [25]. More recently, it has also become clear that socioeconomic status and Medicare coverage are important barriers for people who are willing – but not currently using – PrEP [26].
In addition, as the number of people who are enthusiastic about PrEP have increasingly taken it up, the number of new people initiating PrEP has started to tail off – and in fact has progressively decreased every reporting period since 2018. And this trend was exacerbated (albeit temporarily) during the first year of the COVID-19 pandemic. In the June quarter of 2020 the number of individuals initiating PrEP fell by almost half (45%) compared to the previous quarter, due to COVID-19 and related restrictions [14]. Also, for the first time since PBS listing, the total number of individuals estimated to be taking PrEP declined during the June quarter to 23,428 people from around 25,000 people in the March quarter. Data on PrEP prescriptions in early 2021 suggest that the number of people using PrEP has returned to levels seen in the period prior to the COVID-19 pandemic in early 2020.
As the number of new PrEP users has started to plateau in Australia, more attention has been given to the reasons people discontinue PrEP after having commenced. Research from the United States covering the years 2016 to 2018 suggests that up to a third of gay and bisexual men who commenced PrEP, subsequently discontinued [27]. Similarly, in Australia 30% of participants in EPIC-NSW discontinued PrEP over two years of follow-up (with 85% not recommencing during that time) [28], and in the PrEPX study in Victoria, 25% of participants discontinued PrEP during follow-up, and 78% of these did not recommence use [3].
It is therefore important to identify the reasons for discontinuation in order to determine if any of these reasons can be addressed through interventions. The most commonly cited reasons for stopping – either temporarily or permanently – include: having less sex [19, 29, 30]; no longer being at risk (or reassessing risk) [3, 19, 28, 30-34]; entering a relationship (with an agreement about HIV and/or sex with other partners) [19, 34-36]; experiencing side effects from the medication [31, 37]; and having concerns about taking medication [19, 31, 35]. Other issues associated with discontinuation include substance use [3, 34, 38], and mental health status and housing loss [34, 38]. In terms of other socio-demographic factors, younger age has been strongly associated with discontinuing PrEP [3, 22, 24, 30, 31, 33, 36], as well as non-urban location (of doctor and/or patient) [22]. Also, in Australia, women are more likely to discontinue PrEP after initiating [22].
While affordability issues (including the cost of PrEP, insurance coverage, cost and time of medical visits) were common in literature from the US [33, 34, 38, 39] they have not been a strong feature in Australian studies. However, lack of Medicare coverage has increasingly emerged as a significant issue [23], albeit in relation to people accessing PrEP in the first place rather than in relation to discontinuation. However, people not covered by Medicare are still currently eligible to access public sexual health clinics to receive a prescription for PrEP and for ongoing clinical monitoring.
Another issue that has been identified in Australia (albeit in the era of implementation studies) is that people who were referred for PrEP by a clinician were more likely to discontinue compared to those who self-referred [36]. Similar findings have also been reported elsewhere, which suggests that more work needs to be done to align prescribing practices with the needs of patients/clients, and to avoid prescribing unwanted interventions – although also ensuring that support is in place for people who want to use PrEP but have difficulties in persevering.
Research has also shown that discontinuing or pausing PrEP does not always occur after careful consideration, especially with regards to stopping after commencing a new relationship. Decisions to stop PrEP can be sudden – sometimes not appearing to be decisions at all – and even in the context of starting a new relationship, discontinuing PrEP can occur with little discussion [35]. It is also very unusual for people discontinuing PrEP due to a new relationship to discuss this intention with clinicians. As a clinician at AFAO’s 2020 webinar on stopping, pausing and restarting PrEP noted:
What I find in my clinical practice is that people stop PrEP in the context of starting a new relationship and the feeling that their HIV risk in that relationship is low. But I tend to always find out retrospectively. It’s very uncommon for people to come into the clinic and say, ‘Look, I’m thinking of stopping PrEP, so what should I do, how should I do it?’ It’s very much they come in for something else – an STI screen or something unrelated – and it turns out that they’ve stopped.
I have argued elsewhere that reframing PrEP in ways that correspond to the concerns of users is vital in order to support people’s decisions around PrEP use [35]. Promoting a shared decision-making approach is also important [40]. People generally make decisions about discontinuation, temporary breaks, and re-initiation of PrEP not in the clinic, but on their own, or with their partners, at home. Reframing PrEP around users’ concerns would also emphasise that PrEP isn’t only a clinical intervention, but is rather a social practice – the majority of which occurs outside the clinic. And therefore, peer support and community education about PrEP are just as important as clinical care.
The COVID-19 pandemic provided an unexpected natural experiment in which to observe patterns of discontinuation and re-initiation of PrEP. Studies conducted over the early period of the pandemic in numerous countries have shown that many men suspended their use of PrEP, primarily because they were not having sex during this time [29, 41-44]. This trend was most dramatic in the UK where two-thirds of the men who had been taking PrEP before the COVID-19 outbreak, suspended their PrEP use [44]. In Australia, 41.8% of the men who had been taking PrEP suspended their PrEP use during the early period of COVID-19 restrictions [29].
Regulatory/access issues
Citizens and permanent residents of Australia have access to the national health insurance program, Medicare, and to subsidised medicines through the Pharmaceutical Benefits Scheme (PBS). Since April 2018, co-formulated tenofovir disoproxil and emtricitabine has been subsidised for use as PrEP. PrEP can now also be prescribed by all general practitioners, medical specialists, and accredited nurse practitioners.
Since January 2021, changes to the PBS criteria for prescribing PrEP removed the age restriction to allow prescribing for individuals under 18 years of age, as well as expanding the window for a negative HIV test result before initiation to 4 weeks (assisting access for rural and remote patients), and removed the high and medium HIV risk categories, aligning them with the PrEP suitability criteria in the 2019 updated ASHM PrEP guidelines [45].
The revised 2019 ASHM guidelines also introduced a new concept where a person was not required to have past HIV acquisition risk, as long as they anticipated having future HIV acquisition risk in the next three months. This change to PrEP clinical guidance (in 2019) [45] away from ‘eligibility’ determined by risk categories and towards a framing that highlights ‘suitability’ for PrEP may offer new possibilities for different modes of engagement between clinicians and clients (albeit with suitability still being largely decided by experts). The new guidance on discussing discontinuation and re-initiation and event-based strategies at the time of starting PrEP also offers some different possibilities for engagement within the clinic. A clinician who spoke at AFAO’s 2020 webinar on stopping, pausing and restarting PrEP described the influence of the guidance on clinical practice:
There’s much more of an emphasis that when clinicians assist someone to start on PrEP, they should at the outset, if that patient is someone who falls into the population group for whom on-demand PrEP may also be a suitable method of PrEP, then it is recommended that that’s discussed with that person at the time of starting PrEP and that they’re given appropriate education around on-demand PrEP.
In addition to event-based dosing, there was also an opportunity to discuss both discontinuation and re-initiation of PrEP:
And the other thing that’s highlighted more strongly in the latest version of the guidelines and the resources is that when the clinician is talking to a patient about starting PrEP or during their ongoing monitoring visits, it’s really important that they also talk about under what circumstances someone might consider stopping PrEP and what their plans would be for stopping PrEP safely and what their plans would be for subsequently restarting PrEP if their situation changes.
These ASHM guideline changes have contributed to making PrEP more widely available in Australia. However, a number of impediments to accessing PrEP remain for people without Medicare coverage – including access to clinical care, pathology testing, and pharmaceuticals. Also, not all jurisdictions or research bodies will permit people without Medicare coverage to enrol in clinical studies, thereby impeding both access to PrEP and collection of data on which PrEP modalities are best suited to people living and working in Australia without full residential status.
Some local, state, and community-led solutions (or workarounds) have been developed to address the issue of PrEP access for people not covered by Medicare. However, these solutions operate with different levels of certainty and are, in general, not widely promoted. One of these projects is the PrEP-ME clinic in Victoria [46] for people not covered by Medicare. One of the founders of the clinic described the model in the following way at a recent AFAO webinar:
We have advertised it with colleagues to people who are here. They don’t have a Medicare card. […] They do have private insurance because a lot of them are either working here or they’re studying. So, they’re on the visas which carry requirements around having some other sort of health insurance. […] It’s a nurse-led clinic and [the hospital has] given us the green light to have a clinic with people without Medicare. So, we are really trying to support people who we worry would not be picked up or would not want to go to another clinic.
Work is also currently being undertaken with university health services in Victoria in an attempt to get them to reproduce the model of PrEP-ME. In New South Wales, the MI-EPIC (Medicare Ineligible) study provided access to PrEP for people not covered by Medicare. For all such models, however, the cost of clinical consultations and pathology testing need to be absorbed by the individual services, institutions, and laboratories, and/or the health department of the state or territory.
Once prescribed PrEP, people without Medicare coverage can also access the drugs by importing them directly from offshore pharmaceutical manufacturers or distributors. However, it is also important to note that people’s ability to navigate this system – for example the websites and payment systems of these providers – varies greatly, and may be particularly difficult for people who have limited English-language skills. Several community groups, services, and businesses have evolved to facilitate this personal-importation option. The first of these groups emerged around the time of the first PrEP demonstration projects in Australia [47], to provide options for people wanting to access PrEP who were not participating in these projects, which at the time comprised only a few hundred participants.
One of the Australian community groups, PAN [PrEP Access Now], which emerged in 2015, continues to operate an assistance scheme for people on a low income or who are experiencing financial hardship. Also, even in the period of the early PrEP demonstration projects, organisations such as ACON, AFAO and THH were providing information about personal importation on their websites. The Therapeutic Goods Administration (TGA) regulations allow personal importation via ‘off-label’ prescribing of a drug or drug combination that is already approved. People can import up to 3-months’ supply of pharmaceuticals for which they have a valid prescription.
In the United Kingdom, similar community-based PrEP groups emerged to promote and facilitate access to PrEP through personal importation for those not participating in an early PrEP study, as well as those in the study who were facing loss of access to PrEP once the study ended [48]. As one informant who was involved in PrEP activism, recalled:
People started coming along and saying we’re really worried about what’s going on with PrEP and we’re worried about a lack of activism, we’re worried that no one’s putting any pressure on Gilead. The PROUD trial was coming to an end, and there were 550 guys who had been regularly using PrEP who were being told that they would no longer access PrEP.
One issue of concern regarding personal importation, however, is the degree to which these PrEP users are monitored for STIs and HIV as well as for adverse effects such as changes in kidney function and bone mineral density compared to consumers who access PrEP locally. A PrEP activist from the UK interviewed for this essay noted that in that country, ‘People who bought PrEP online – versus people who accessed PrEP on the Impact trial – were less likely to have regular STI tests and HIV tests’. A comparison between these groups in Australia would be interesting, but the relatively small number of personal importers in Australia makes such a comparison difficult.
There are of course also issues regarding access even in a local-prescribing context. Some prescribers for example are hesitant to prescribe PrEP solely to alleviate what they perceive to be ‘HIV anxiety’ [49]. Prescribing PrEP for HIV anxiety is currently endorsed by the ASHM guidelines on a case-by-case basis. Experienced prescribers have also expressed concerns about the competence of non-specialist GPs in discussing sexuality with patients [50].
The design of clinical services is also likely to be an important factor in facilitating continued use of PrEP as well as facilitating take up among potential new groups. Research from the US for example has identified a number of factors that support ongoing use of PrEP as well as uptake by new users, including drop-in visits, adherence support/counselling, and standing orders for pathology testing [38]. Also important in that context were referrals for services related to housing, substance use, and mental health. Other useful strategies identified in US research include peer navigation [51, 52] and the use of community-informed language for particular groups [53].
Historical issues
As already described, PrEP initially became available in Australia through demonstration projects and implementation studies. Whereas Dodds argues that the Impact trial in England served as a ‘stop-gap’ solution (or ‘show trial’) that was intended ‘to help manage a policy and financial impasse’ and to manage demand for PrEP [54], the Australian studies were intended to provide access to PrEP in the period prior to PBS subsidisation, and also to provide data on the feasibility and impact of providing PrEP through clinical services. The EPIC and PrEPX studies (figs. 1 and 2) were also designed to measure population level benefits of PrEP on HIV notifications. However, this specific history has undoubtedly been influential in defining the shape of PrEP in this country.

Fig. 1. Politicians, researchers, and community representatives at an EPIC-NSW event. The signs they are holding read: ‘PrEP prevents HIV’.

Fig. 2. Staff at community health services in regional Victoria promoting the PrEPX study.
An important feature of the PrEP studies in Australia – and therefore the history of PrEP is this country – is the prominence of daily dosing strategies. Similar to the United States, when regulatory approval for PrEP was granted by the TGA (in 2016) it was for daily dosing only. Currently, non-daily dosing has only been endorsed via the ASHM guidelines, although clinicians can prescribe event-based PrEP on an off-label basis.
The history of PrEP in Europe has been somewhat different. The Ipergay study, conducted primarily in France, investigated an event-based dosing strategy. That study reported in 2015, showing that event-based dosing of PrEP was as efficacious as daily dosing for MSM [55, 56]. Following the Ipergay results, event-based dosing became as common as daily dosing among gay men in France and other continental European countries. A clinician who took part in a recent AFAO webinar on PrEP noted the effects of these different national PrEP histories.
In Australia […] there’s been a preference for daily PrEP. […] In France, […] they’ve only ever had on-demand PrEP. They’ve never had a daily PrEP program. And the PrEP preference amongst French men who have sex with men is very much for on-demand PrEP, not daily PrEP.
These ‘preferences’ can also be understood as a result of the ways in which different strategies were preferentially emphasised in different national contexts. The same clinician (from above) noted that this strong historical emphasis on daily dosing in Australia may contribute to a lack of confidence in event-based dosing, a fact which has been noted in local research [57].
We’ve always had a very strong emphasis on daily PrEP and rightly so […] but it then makes it then really difficult to mentally reconcile that with a method like on-demand PrEP, where you know all of a sudden say, okay, well, either you should take it every day or if you don’t want to, you could choose to take two tablets at least two hours before sex and then one tablet 24 hours later, [and then another tablet 24 hours after that]. So, it’s a very different message.
The history of PrEP in Australia, which I have argued has led to daily PrEP dosing being the predominant strategy, may also have contributed to PrEP users being less skilled in linking their PrEP use with (un)anticipated sexual encounters. Clinicians too, are also plausibly less skilled in prescribing and monitoring on-demand PrEP. The COVID-19 pandemic has therefore perhaps encouraged previous daily users to consider other PrEP dosing regimens for the first time. This experience might be useful in popularising other dosing regimens.
There is already evidence to suggest that both users and non-users are very interested in long-acting injections and implants, and that daily dosing isn’t that popular – even if that was the main way users were taking it [19, 58, 59]. In one national survey, a quarter (26.5%) of gay and bisexual men not currently taking PrEP reported they would prefer event-based dosing, compared to only 8.4% of those who were currently taking PrEP [19]. A NSW survey of current and previous PrEP users who had been part of an earlier PrEP clinical trial found that 42.8% were interested in event-driven PrEP [59]. A similar Victorian survey of current and previous PrEP users also found that almost half (48%) would be willing to switch to event-based dosing [58]. Those who were interested in event-based dosing were more likely to have discontinued PrEP, to have sex infrequently, to have difficulty with adherence, or to have concerns about toxicity. These findings strongly suggest that event-based PREP strategies may appeal to some men who are already taking daily PrEP, and may perhaps be even more appealing to potential new users (i.e. people not currently taking PrEP).
In addition to the history of PrEP in Australia leading to a predominance of daily dosing, it could also be argued that the ways in which PrEP was initially rolled out favoured particular (potential) consumers [60]. For example, the ‘early adopters’ who participated in demonstration projects (from 2014 to 2016) – as well as those involved in activism around personal importation – were not only those who were the most sexually active [2, 6, 21, 61], but were also largely men who were had some knowledge of PrEP and were to connected to services and/or community organisations [21].
As a result of availability in Australia emerging primarily through implementation studies (and personal importation), PrEP has been disproportionately taken up by older, Australian-born, non-Indigenous, gay-identified men, living in metropolitan areas, and those with higher socioeconomic status [23]. As recent analyses of PrEP use among men in NSW show, PrEP use is still strongly associated with self-identifying as gay, living in an area in which there is a higher proportion of residents who identify as ‘gay’, and being aged over 25 years [15]. The combination of these factors – especially residential location and age – greatly increases the likelihood of being on PrEP, with 74% of high-risk men who are aged over 25 years and live in a ‘gay’ suburb being on PrEP, which is more than double the proportion (34%) of high-risk men on PrEP who are aged under 25 years and live in a ‘non-gay’ suburb [15].
These findings related to residential location also mask other important factors, particularly those related to socio-economic status. At a national level, PrEP users – compared to willing non-users – are more likely to be employed full-time (73% vs. 54%), have a higher income, be university educated, and be covered by Medicare [23]. Also. the ‘gay’ postcodes in NSW specifically, where the definition refers to postcodes in which more than 20% of residents identify as gay are primarily areas in which residents have access to more material, social and cultural resources in general.
Also, as noted in the recent NSW report referred to above, men living in areas in which more than 20% of residents identify as gay tend to have more direct social engagement with other gay men, which suggests that social norms (including perceived norms) among peers may be an important factor in uptake and maintenance of PrEP. Nationally, PrEP use is also associated with social norms, specifically being more likely to have sex with others on PrEP, and to know people living with HIV (PLHIV) [23]. This emphasis on social norms was also noted Quinn et al.’s exploration of the role of opinion leaders in influencing PrEP use in Black LGBT communities in the United States [62]. Similarly, Holt et al.’s analysis of PrEP uptake in Australia explicitly focuses on the social processes involved in the uptake of PrEP at a community level [21]. This analysis explains the pattern of PrEP uptake using a Diffusion of Innovations perspective, which is a theory that has been developed to predict how over time, an idea or product gains momentum and spreads through a specific population or social system.
As described above, PrEP use among men in NSW is strongly associated with residential location and age. Nationally, PrEP use is associated with having Medicare coverage, in addition to other factors related to men’s social and sexual connections – such as knowing any PLHIV, having a greater number of sexual encounters, and having more involvement with other PrEP users [23]. However, the association between PrEP use and country of birth is less strong. In NSW, for example, PrEP use among overseas-born men aged over 25 years is similar to PrEP use among Australian-born men in the same age group [15].
PrEP use is however related to other factors, some of which intersect with cultural background, such as sexual identity [16, 63]. Research among overseas-born men has identified a number of issues related to PrEP uptake. Recent research among overseas-born men recently diagnosed with HIV found that even though these men generally considered PrEP a positive strategy, they did not necessarily consider it appropriate for them personally because they did not see themselves as sufficiently high risk [64]. Similarly, recent market research identified a range of factors contributing to not taking PrEP, including perceived individual risk, beliefs about HIV prevalence in Australia, concerns about the impact of HIV testing on visa status, knowing how to navigate the health system, attitudes towards PrEP, cultural influences on sexuality, and cost including for doctor’s consultation for those not covered by Medicare [65].
Demand creation
The previous sections have explored some the reasons for discontinuation of PrEP, as well as historical factors and the material barriers (including socio-demographic factors) associated with uptake (or non-uptake) of PrEP. This section considers some of the ways in which the users – or consumers – of PrEP are imagined or constructed through activities such as activism and health promotion, including some reflections on the theoretical approaches used, and the kinds of benefits that are drawn on to promote PrEP use. It includes an analysis of selected health-promotion messaging regarding PrEP, and also draws in part on the expertise of those who have been involved in the development of this work. The analysis draws on a domain of the HIV prevention cascade framework – demand – and specifically, demand creation [66, 67]. It has been argued that there is not currently a very extensive literature on demand creation, and that user-centred design and demand-side thinking has been unevenly applied [68].
While there has been an understandable focus on the socio-demographic factors associated with the uptake (or non-uptake) of PrEP, identifying these factors does not, on its own, provide solutions in terms of increasing uptake (or even awareness) among the sub-groups identified, such as younger gay and bisexual men. Attitudinal factors – some of which, such as perceived risk, and concerns about the ongoing use of antiretrovirals [69] – have already been mentioned, and perceived social norms, are important in the design of interventions. In fact, as argued by Holt (2015), when technologies such as PrEP are designed, ‘potential users are typically defined, enabled and constrained, partly to create a target population (or market) for the technology, but also to reassure people that it can be used safely and effectively’ [60]. Such configurations may be more or less useful as PrEP is rolled out, and as Holt notes, the initial focus on HIV risk in thinking about the ultimate user of PrEP during the period of its development may be an important factor in non-uptake among some groups. Some US researchers have provided some suggestions for ‘next-wave PrEP implementation efforts’ that move beyond a focus on risk [70]. In addition to redefining PrEP eligibility assessments, these strategies include de-emphasising risk perception, discarding risk compensation arguments, making PrEP follow-up less arduous, and reducing costs [70].
It is clear from examining some of the messaging in Australian PrEP health-promotion campaigns – as well as discussion with people involved in the development of these messages – that, over time, there has been a progression from discreet and targeted messaging to those who were at high risk of HIV acquisition (by way of their sexual practices involving condomless sex with unknown-status partners), towards more explicit promotion of PrEP, and its potential benefits, to prospective users. This progression is evident in ACON’s campaigns and messaging. This messaging started with recruitment for the EPIC Study (‘PrEP prevents HIV’ [fig. 1]), and was followed later in 2016 with the messaging, ‘Is PrEP for you?’, and then the ‘How do you do it?’ campaign (figs. 3–5) was launched in 2017. The campaign promoted what could perhaps be called equivalent prevention, that is the comparability of condoms, PrEP and UVL. The latest (and current) campaign, ‘Take me…’ (fig. 11) began in early 2021 focuses on different PrEP dosing strategies (daily, intermittent, and event-based dosing).
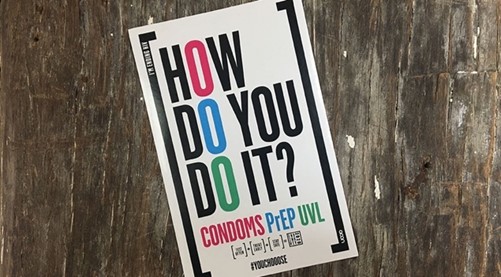
Fig. 3. An image from ACON’s ‘How do you do it?’ campaign showing the equal emphasis on condoms, PrEP, and UVL.

Fig 4. Outdoor posters of ACON’s ‘How do you do it?’ campaign.
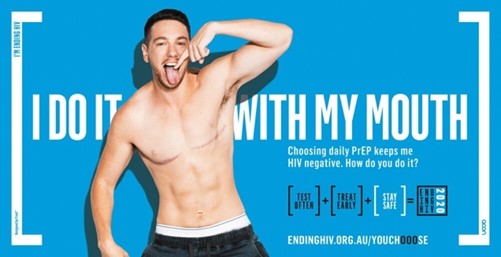
Fig 5. A billboard from ACON’s ‘How do you do it?’ campaign showing the PrEP messaging. The text reads: ‘I do it with my mouth. Choosing daily PrEP keeps me HIV negative. How do you do it?’
The first generation of messaging (in 2016) was produced in the context of possible community resistance to PrEP in terms of undermining condom use as one informant involved in the development the first messaging noted, ‘We were very much aware of the Truvada wars that then stemmed from the States’. Following that early, tentative, period, there was a focus on consumption-based strategies that were interested in creating attachments to PrEP and in equivalence between PrEP, condoms and treatment-as-prevention as strategies, as well as emphasising consumer choice in terms of selecting between these strategies (see ACON’s ‘How do you do it?’ campaign [(figs. 3–5]). The PrEP messaging comprises the following: ‘I do it with my mouth. Choosing daily PrEP keeps me HIV negative. How do you do it?’ (fig. 11). As an informant who was involved in the development of these campaigns described:
We wanted to be able to promote each HIV prevention strategy equally, so as not to pit one against the other. We didn’t want to say that condoms were more effective. We didn’t want to say PrEP or UVL [undetectable viral load] was more effective. And so, we went with the language of ‘highly effective at preventing HIV’.
In addition to emphasising agnosticism regarding the choice of prevention strategies, the campaign also focused on their interchangeability.
We wanted to talk about the complexity of how one person may use one strategy, another person may use another, but that’s okay. And they work together. We wanted to talk about how you can switch between strategies – just because you make a decision now doesn’t mean that you can’t change that later on.
Similarly, it is possible to see a progression from Thorne Harbour Health’s early information-based campaign, ‘10 things you need to know about PrEP’ (fig. 6), to their later recent ‘What works’ campaign (fig. 7). Like ACON’s ‘How do you do it?’ campaign, ‘What works’ emphasised that PrEP, condoms and the use of undetectable viral load were all effective ways of preventing HIV.
Fig. 6. An image from an early information-based campaign, ‘10 things you need to know about PrEP’, from the Victorian AIDS Council (now Thorne Harbour Health).

Fig 7. A screenshot from Thorne Harbour Health’s campaign, ‘What works’ campaign showing the PrEP messaging. The text reads: ‘I take PrEP to avoid HIV. That’s what works for me’.
Another important aspect of PrEP campaigns was to raise awareness and competence related to PrEP among particular groups of gay and other men who have sex with men. AFAO’s 2019 ‘Get PrEP’D’ campaign (figs. 8 and 9), for example, promoted PrEP among men from Indigenous and culturally or linguistically diverse backgrounds, as well as men and masc people of trans experience. The campaign addressed specific barriers experienced by these groups that had been identified in research and market testing [65]. Another feature of this campaign, as well as Queensland AIDS Council’s ‘ComePrepd’ campaign (fig. 10) was its messaging for people living outside large urban centres.

Fig. 8. An image from ‘Get PrEP’D’, AFAO’s PrEP campaign for gay, bisexual and other men (cis or trans), non-binary inclusive, who have sex with men.

Fig. 9. A scene from one of the videos from AFAO’s ‘Get PrEP’D’ campaign.

Fig. 10. An image from Queensland AIDS Council’s ‘ComePrepd’, a community-driven HIV prevention campaign to increase awareness of PrEP. www.comeprepd.info/category/stories/.
As findings from regular surveys of gay men from across the country revealed PrEP’s increasing popularity – ultimately emerging as the most common prevention strategy for HIV-negative gay men [71] – messaging related to PrEP has become confident. This style is evident in ACON’s current ‘Take me…’ campaign (fig. 11), which focuses on different models of PrEP (or different dosing strategies). The ‘Take me…’ PrEP campaign also invites men to identify the most appropriate dosing strategy for them ‘based on identity, the type of sex they have, how often they hook-up, and personal preference’ [72].
A significant shift in this campaign compared to its predecessors is the focus on the pill itself, including the decision to make the pill the subject of the campaign messages. This shift in subjectivity is evidenced by the pill speaking directly to the reader, ‘Take me’, compared to previous campaigns, which tended to refer to PrEP using the pronoun, ‘it’. This explicit focus on the relationship between the pill (or PrEP) is also interesting because it invites the reader to think about PrEP relationally, and the contexts in which it might be appropriate – and moves away from a more clinical framing.
These different phases of PrEP health promotion have also been characterised by demand-creation strategies and approaches that draw on, or evoke, different affective responses. The earliest messages, including those that accompanied the EPIC study, focused on building confidence in PrEP. Building confidence at that time meant using specific messaging that emphasised PrEP’s effectiveness, thereby reducing concerns about sex in the absence of condoms as well as emphasising the idea of a real choice between different HIV prevention options, which was also a novel idea at that point.

Fig. 11. An image from ACON’s ‘Take me’ PrEP campaign.
Fig. 12. A scene from Thorne Harbour Health’s video about on-demand PrEP.
Later messaging focused on reduction of fear and anxiety related to HIV and sex. And in more recent times, other affective responses were deliberately drawn on – those that focused explicitly on the pleasures and intensities associated with condomless sex. As one health-promotion informant from NSW put it, campaigns began to focus on ‘the emotion, the feeling that people have, the pleasure, which I think is a really important part of being able to fuck without a condom’. This strategy was adopted in contrast to other approaches around the same time that talked about PrEP ‘being 98% effective, 99% effective’, according to the same informant, which far from creating confidence, actually ‘leaves doubt’.
The pleasures and intensities of condomless sex were are also directly invoked in the earlier ‘FUCK RAW’ (fig. 13) messaging of ‘a guerrilla poster campaign’ that appeared in Melbourne’s inner city in September 2015 [47]. Borrowing from the tactics of early AIDS activism the campaign’s ‘celebration of condomless anal sex, was designed to cause controversy, raise awareness of HIV pre-exposure prophylaxis (PrEP), and challenge the authority of already-established HIV/AIDS organisations’ [47].

Fig. 13 An image from the guerrilla poster campaign that appeared in Melbourne in September 2015. The poster reads, ‘YOU CAN FUCK RAW. PrEP WORKS. NO MORE HIV’.
It’s perhaps more difficult to identify the specific affective appeals in the current PrEP campaigns, those promoting alternate dosing strategies such as event-based and intermittent PrEP like the ‘Take me…’ campaign from ACON (fig. 11) and THH’s video ‘What’s on-demand PrEP?’ (fig. 12). Certainly, the visual imagery is imbued with playful qualities and the text has a sense of lightness despite taking the command form. And these qualities seem to match well with the thinking behind the campaign, which, as described earlier, intended to emphasise the ease with which users could swap between these different strategies.
In addition to appeals that have been used in current and previous health-promotion messaging, work undertaken by researchers, health-promotion practitioners, and activists, has identified a range of factors that might be drawn on in developing strategies to promote PrEP. In particular, they identify possibilities for promoting the idea of PrEP as a viable and relevant strategy, for people who might benefit from it, but are not currently using it, and to prevent discontinuation among those who are still at risk of HIV infection, by emphasising specific (anticipated or promised) effects.
Australian studies have noted how PrEP users have experienced reduced HIV concern and increased pleasure and intimacy in their sexual encounters (as a result of adopting this technology) [21, 73], and also specific forms of intensification associated with condomless sex [73]. The findings of Wells’ study of PrEP users in Victoria also drew attention to the fact that PrEP was particularly meaningful for men who take the receptive role during anal sex and wanted to achieve a greater sense of control over HIV prevention – whereas they had not always felt able to ensure that their sex partners used condoms [73].
Other Australian (and international) research has identified that PrEP users experience decreased levels of concern or ‘anxiety’ related to HIV and sex compared to the period before starting to use the technology [24, 74]. These affective aspects of PrEP provide useful tools for thinking about strategies that could be used to promote PrEP among at-risk groups with low levels of consumption, however they will not overcome access issues related to non-coverage by Medicare (including newly arrived residents and international students).
Health promotion and activism efforts have, to date, focused on creation of awareness about PrEP, but arguably have not paid as much attention to creating demand among specific groups – a task that is now more pressing as the majority of those who were predisposed, or motivated, to take, PrEP, have already taken it up. Attitudes to PrEP among this remaining group are more likely to be negative [19], suggesting that they will require different strategies to convince them to take PrEP – if they can be convinced at all – and therefore whether different PrEP modalities, such as long-acting injectables, may be more attractive.
Health promotion strategies to date have been based on a limited number of approaches, such as information-based models, and have drawn on consumption-based theories, including Diffusion of Innovations [21]. While the latter provides a model for predicting the uptake of new technologies or innovations in a population it is not necessarily well suited to identifying the reasons for doing so. However, some ideas for strategies to increase uptake among potential users are provided in recent research. For example, a recent study in the US found that initiating PrEP while on vacation could be a means for transitioning to long-term use [26].
One wonders also whether instead of promoting different dosing strategies as different versions of the same strategy, whether it would be possible instead to think about these strategies as different strategies – or objects? While emphasising ‘different ways’ to take PrEP may facilitate moving between them, and make non-daily strategies seem less exotic, this emphasis may diminish the possibility of creating attachments to specific strategies by suggesting they are all different versions of the same thing.
Also, some of the newer ways of consuming PrEP that are on the horizon, such as long-acting injectables and implants might be leveraged as a way of creating interests in current PrEP strategies – for example, why not try daily or on-demand PrEP while you’re waiting for better options?
Discussion
The first section of this essay provided an overview of practical and regulatory issues related to PrEP access. Since 2018, when the antiretroviral drugs used for PrEP were listed on the PBS for HIV prevention, citizens and permanent residents of Australia (i.e. those with Medicare coverage) have had access to PrEP. PrEP uptake has also been facilitated by national and state HIV strategies, which have ambitious targets regarding PrEP coverage, and clinical guidance documents that encourage health-care providers to discuss PrEP with suitable patients.
However, as has been well documented, no satisfactorily ongoing solution has yet been found for people not covered by Medicare (including newly arrived residents and international students) although several small-scale access programs exist at state and local level. It is worth noting however that federal funding has recently been secured for antiretroviral therapy for PLHIV not covered by Medicare. And although not discussed within this essay, it is also worth noting that modelling studies from the Netherlands and the UK for example have found that PrEP is cost-effective and even cost-saving [75, 76]. The national benefit of such a policy is also clear, in the sense that PrEP provision would contribute to suppressing new infections in the community.
Historical issues related to PrEP were also covered. The way in which PrEP became available in Australia – via clinical demonstration projects and personal importation of generic medications, prior to TGA approval and PBS listing – has led to an emphasis on daily dosing strategies (similar to the United States, but in contrast to several Western European countries where event-based strategies are more the norm). This focus on daily PrEP may have prevented uptake by those who have infrequent sexual contacts and/or concerns about toxicity both of which have also been identified as reasons for discontinuing PrEP. Finally, the essay sought to provide some insights into public messaging about PrEP, specifically messages developed by community-based HIV and LGBTQ health organisations, and to reflect on some of the approaches that these campaigns draw on.
Given the current national/global focus on COVID-19 vaccination intentions, it seems appropriate to draw on a WHO model for immunisation, despite its psychological origins, to think about PrEP uptake [77], and in particular, the demand-creation approach [68] used in this essay. In this model, ‘motivation’ (or readiness, willingness, intention, hesitancy) is made up of two components: 1) what people think and feel (perceived risk, worry confidence, trust and safety concerns); and 2) social processes (provider recommendation, social norms, gender norms and equity, information sharing, rumours). Motivation only leads to vaccination or PrEP uptake in this case, however, if practical issues are also addressed. These issues comprise availability, convenience, costs, requirements, and incentives. The most effective interventions are those that seek to leverage, but not change, what people think and feel. There is a range of ways in which these interventions can build on existing favourable intentions. One of these is to facilitate action (through reminders, prompts, and primes). Another is to reduce barriers (through logistics and healthy defaults). And the final one is to shape behaviour (through incentives, disincentives, and requirements).
This model may provide a way of thinking about the different factors that contribute to uptake of particular technologies or interventions, such as PrEP (although certain distinctions must of course be noted, for example, that PrEP, unlike immunisation, is an ongoing intervention. Regardless, this essay has sought to analyse the current and historical factors that have influenced –and continue to influence – PrEP access, uptake, and persistence, in Australia. These factors, along with the specific individuals and communities that are affected by HIV in this country, make up PrEP in Australia as a particular object – the specifics of which should therefore remain an important consideration.
References
- AFAO, Agenda 2025: Ending HIV Transmission In Australia (Technical paper on science, trends and targets). 2021: Sydney.
- Lal, L., et al., Medication adherence, condom use and sexually transmitted infections in Australian preexposure prophylaxis users. AIDS, 2017. 31(12): p. 1709-1714.
- Ryan, K., et al., Results from a large Australian PrEP demonstration study: Discontinuation and subsequent HIV and other sexually transmitted infection risk, in Tenth International AIDS Society Conference on HIV Science. 2019: Mexico City.
- Kirby Institute, Monitoring HIV pre exposure prophylaxis uptake in Australia: PBS-subsidised HIV Pre-exposure Prophylaxis from April 2018 to June 2020. 2019.
- Zablotska, I.B., et al., The estimated number of potential PrEP users among gay-identifying men who have sex with men in Australia. PLOS ONE, 2018. 13(10): p. e0204138.
- Vaccher, S., et al., Protocol for an open-label, single-arm trial of HIV pre-exposure prophylaxis (PrEP) among people at high risk of HIV infection: the NSW Demonstration Project PRELUDE. BMJ open, 2016. 6(6): p. e012179.
- Grulich, A.E., et al., Population-level effectiveness of rapid, targeted, high-coverage roll-out of HIV pre-exposure prophylaxis in men who have sex with men: the EPIC-NSW prospective cohort study. Lancet HIV, 2018. 5(11): p. e629-e637.
- Ryan, K.E., et al., Protocol for an HIV Pre-exposure Prophylaxis (PrEP) Population Level Intervention Study in Victoria Australia: The PrEPX Study. Front Public Health, 2018. 6: p. 151.
- Ryan, K., et al., Population level decline in incident HIV infection among gay and bisexual men following scale-up of PrEP in Victoria, Australia, in Australasian HIV/AIDS and Sexual Health Conference. 2020: Virtual.
- Kirby Institute, National HIV Quarterly Notifications Data. 2021.
- Kirby Institute, HIV, viral hepatitis and sexually transmissible infections in Australia: annual surveillance report 2018. 2018, Kirby Institute, UNSW Sydney: Sydney.
- Gunaratnam, P., et al., HIV diagnoses in migrant populations in Australia—A changing epidemiology. PLOS ONE, 2019. 14(2): p. e0212268.
- Medland, N.A., et al., Incident HIV infection has fallen rapidly in men who have sex with men in Melbourne, Australia (2013–2017) but not in the newly-arrived Asian-born. BMC Infectious Diseases, 2018. 18(1): p. 410.
- Kirby Institute, Monitoring HIV pre exposure prophylaxis uptake in Australia: PBS-subsidised HIV Pre-exposure Prophylaxis from April 2018 to June 2020. 2020.
- Grulich, A., et al., Trends in HIV and HIV prevention indicators in gay, bisexual and other men who have sex with men in NSW, 2015-2019: implications for new interventions and for monitoring and evaluation in a new NSW HIV strategy. 2020, Kirby Institute, UNSW Sydney Sydney.
- Hammoud, M.A., et al., HIV Pre-exposure Prophylaxis (PrEP) Uptake Among Gay and Bisexual Men in Australia and Factors Associated With the Nonuse of PrEP Among Eligible Men: Results From a Prospective Cohort Study. JAIDS Journal of Acquired Immune Deficiency Syndromes, 2019. 81(3): p. e73-e84.
- Meanley, S., et al., Assessing the Role of Gay Community Attachment, Stigma, and PrEP Stereotypes on Young Men Who Have Sex with Men’s PrEP Uptake. AIDS and behavior, 2021. 25(6): p. 1761-1776.
- Thomann, M., et al., ‘WTF is PrEP?’: attitudes towards pre-exposure prophylaxis among men who have sex with men and transgender women in New York City. Culture, Health & Sexuality, 2018. 20(7): p. 772-786.
- MacGibbon, J., et al., Attitudes to biomedical HIV prevention among Australian gay and bisexual men: Key findings from the PrEPARE Project 2019. Centre for Social Research in Health, UNSW Sydney, Sydney. 2019.
- Annequin, M., et al., Are PrEP services in France reaching all those exposed to HIV who want to take PrEP? MSM respondents who are eligible but not using PrEP (EMIS 2017). AIDS Care, 2020. 32(sup2): p. 47-56.
- Holt, M., et al., Trends in Attitudes to and the Use of HIV Pre-exposure Prophylaxis by Australian Gay and Bisexual Men, 2011-2017: Implications for Further Implementation from a Diffusion of Innovations Perspective. AIDS Behav, 2019. 23(7): p. 1939-1950.
- Medland, N., et al., Successful national PrEP scale-up in Australia: Evaluation of uptake, adherence, discontinuation and HIV seroconversion from April 2018 to September 2019 using national dispensing data, in AIDS2020. 2020: Virtual.
- MacGibbon, J., et al., Access to Subsidized Health Care Affects HIV Pre-Exposure Prophylaxis (PrEP) Uptake Among Gay and Bisexual Men in Australia: Results of National Surveys 2013–2019. JAIDS Journal of Acquired Immune Deficiency Syndromes, 2021. 86(4).
- Whitfield, T.H.F., et al., The Impact of Pre-Exposure Prophylaxis (PrEP) Use on Sexual Anxiety, Satisfaction, and Esteem Among Gay and Bisexual Men. J Sex Res, 2019. 56(9): p. 1128-1135.
- Mwaturura, C., et al., Barriers and facilitators to pre-exposure prophylaxis among African migrants in high income countries: a systematic review. Sexual Health, 2021. 18(2): p. 130-139.
- Egan, J.E., et al., Feasibility of Short-Term PrEP Uptake for Men Who Have Sex With Men With Episodic Periods of Increased HIV Risk. JAIDS Journal of Acquired Immune Deficiency Syndromes, 2020. 84(5).
- Holloway, I.W., et al., Longitudinal trends in PrEP familiarity, attitudes, use and discontinuation among a national probability sample of gay and bisexual men, 2016-2018. PLoS One, 2020. 15(12): p. e0244448.
- Grulich , A., et al., Continuing low HIV incidence in the Expanded Pre-exposure Prophylaxis (PrEP) Implementation in Communities – New South Wales study (EPIC-NSW), in International AIDS Society Conference on HIV Science. 2019: Mexico City, Mexico.
- Hammoud, M., et al., Substantial decline in use of HIV pre-exposure prophylaxis (PrEP) following introduction of COVID-19 physical distancing restrictions in Australia: Results from a prospective observational study of gay and bisexual men. JAIDS Journal of Acquired Immune Deficiency Syndromes, 2020. Publish Ahead of Print.
- Bavinton, B., et al., Factors associated with stopping HIV pre-exposure prophylaxis (PrEP) for three months or more in the EPIC-NSW trial, in International AIDS Society Conference on HIV Science. 2019: Mexico City, Mexico.
- Koppe, U., et al., Barriers to using HIV pre-exposure prophylaxis (PrEP) and sexual behaviour after stopping PrEP: a cross-sectional study in Germany. BMC Public Health, 2021. 21(1): p. 159.
- Whitfield, T.H.F., J.T. Parsons, and H.J. Rendina, Rates of Pre-exposure Prophylaxis Use and Discontinuation Among a Large U.S. National Sample of Sexual Minority Men and Adolescents. Archives of Sexual Behavior, 2020. 49(1): p. 103-112.
- Whitfield, T.H.F., et al., Why I Quit Pre-Exposure Prophylaxis (PrEP)? A Mixed-Method Study Exploring Reasons for PrEP Discontinuation and Potential Re-initiation Among Gay and Bisexual Men. AIDS and Behavior, 2018. 22(11): p. 3566-3575.
- Spinelli, M.A., et al., Missed opportunities to prevent HIV infections among pre-exposure prophylaxis users: a population-based mixed methods study, San Francisco, United States. Journal of the International AIDS Society, 2020. 23(4): p. e25472.
- Murphy, D.A., et al., Anticipated and actual experiences of discontinuing PrEP reflect the ‘imagined futures’ and everyday concerns of gay and bisexual men, rather than HIV risk: Implications for service provision and health promotion, in AIDS 2020: 23rd International AIDS Conference. 2020: Virtual.
- Ryan, K., et al., Reasons and predictors of PrEP cessation or interruption among Victorian, South Australian, and Tasmanian PrEPX study participants, in Australasian HIV/AIDS and Sexual Health Conference. 2019: Perth.
- Zimmermann, H.M., et al., Motives for choosing, switching and stopping daily or event-driven pre-exposure prophylaxis – a qualitative analysis. Journal of the International AIDS Society, 2019. 22(10): p. e25389.
- Laborde, N.D., et al., Understanding PrEP Persistence: Provider and Patient Perspectives. AIDS Behav, 2020.
- Kay, E. and R. Pinto, Is Insurance a Barrier to HIV Preexposure Prophylaxis? Clarifying the Issue. American journal of public health, 2020. 110(1): p. 61-64.
- Meyers, K., et al., Salient Constructs for the Development of Shared Decision-Making Tools for HIV Pre-Exposure Prophylaxis Uptake and Regimen Choice: Behaviors, Behavioral Skills, and Beliefs. AIDS Patient Care and STDs, 2021. 35(6): p. 195-203.
- Fernandes, D.E., P.R.A. Ferreira, and G. Mastroianni Kirsztajn, Pre-exposure prophylaxis during the SARS-CoV-2 pandemic: can PrEP prevent COVID-19-related symptoms? Epidemiology and infection, 2020. 148: p. e231-e231.
- Sousa, A.F.L., et al., Casual sex among MSM during the period of social isolation in the COVID-19 pandemic: Nationwide study in Brazil and Portugal. medRxiv, 2020.
- Sanchez, T.H., et al., Characterizing the Impact of COVID-19 on Men Who Have Sex with Men Across the United States in April, 2020. AIDS and behavior, 2020. 24(7): p. 2024-2032.
- Pebody, R. A quarter of gay men report casual sex during UK lockdown. 2020 11 June 2020 [cited 2020 July 4]; Available from: https://www.aidsmap.com/news/jun-2020/quarter-gay-men-report-casual-sex-during-uk-lockdown.
- ASHM, PrEP Guidelines Update. Prevent HIV by Prescribing PrEP. 2019, The Australasian Society of HIV Viral Hepatitis and Sexual Health Medicine: Sydney.
- Armishaw, J., et al., PrEPMe: Provision of PrEP for overseas-born MSM without Medicare in Melbourne Victoria, in Australasian HIV/AIDS and Sexual Health Cnference. 2020: Virtual.
- Wells, N., Risk, safety, stigma, liberation, and pleasure: The experience of sex in the era of pre-exposure prophylaxis, in General Practice. 2021, Monash University: Melbourne.
- Jones, C., I. Young, and N. Boydell, The People vs the NHS: Biosexual citizenship and hope in stories of PrEP activism. Somatechnics, 2020. 10(2): p. 172-194.
- Smith, A.K.J., et al., Issues Associated With Prescribing HIV Pre-exposure Prophylaxis for HIV Anxiety: A Qualitative Analysis of Australian Providers’ Views. J Assoc Nurses AIDS Care, 2021. 32(1): p. 94-104.
- Smith, A.K.J., et al., Troubling the non-specialist prescription of HIV pre-exposure prophylaxis (PrEP): the views of Australian HIV experts. Health Sociol Rev, 2020. 29(1): p. 62-75.
- Walters, S.M., et al., Considerations for the Design of Pre-exposure Prophylaxis (PrEP) Interventions for Women: Lessons Learned from the Implementation of a Novel PrEP Intervention. AIDS and Behavior, 2021.
- Jaramillo, J., et al., Perceptions of Sexual Risk, PrEP Services, and Peer Navigation Support Among HIV-Negative Latinx and Black Men who have Sex with Men (MSM) Residing in Western Washington. Sexuality Research and Social Policy, 2021.
- Fields, E.L., S.A. Hussen, and D.J. Malebranche, Mind the Gap: HIV Prevention Among Young Black Men Who Have Sex with Men. Current HIV/AIDS Reports, 2020. 17(6): p. 632-642.
- Dodds, C.A., Implementation Science or ‘Show’ Trial?: England’s PrEP Impact Study, in Remaking HIV Prevention in the 21st Century – The Promise of TasP, U=U and PrEP, S. Bernays, et al., Editors. In Press, Springer. p. 1-19.
- Anderson, P.L., J.G. García-Lerma, and W. Heneine, Nondaily preexposure prophylaxis for HIV prevention. Current opinion in HIV and AIDS, 2016. 11(1): p. 94-101.
- Molina, J.-M., et al., On Demand PrEP With Oral TDF-FTC in MSM: Results of the ANRS Ipergay Trial, in CROI. 2015: Seattle, Washington. Abstract Number: 23LB.
- Smith, A.K.J., et al., Challenges of providing HIV pre-exposure prophylaxis across Australian clinics: qualitative insights of clinicians. Sex Health, 2021. 18(2): p. 187-194.
- Cornelisse, V.J., et al., Interest in Switching to On-Demand HIV Pre-Exposure Prophylaxis (PrEP) Among Australian Users of Daily PrEP: An Online Survey. Open Forum Infect Dis, 2019. 6(7): p. ofz287.
- Chan, C., et al., Preferences for Current and Future PrEP Modalities Among PrEP-Experienced Gay and Bisexual Men in Australia. AIDS and Behavior, 2021.
- Holt, M., Configuring the users of new HIV-prevention technologies: the case of HIV pre-exposure prophylaxis. Cult Health Sex, 2015. 17(4): p. 428-39.
- Zablotska, I.B., et al., High adherence to HIV pre-exposure prophylaxis and no HIV seroconversions despite high levels of risk behaviour and STIs: the Australian demonstration study PrELUDE. AIDS and Behavior, 2019. 23(7): p. 1780-1789.
- Quinn, K.G., et al., The Influence of Peers on PrEP Perceptions and Use Among Young Black Gay, Bisexual, and Other Men Who Have Sex with Men: A Qualitative Examination. Archives of Sexual Behavior, 2020. 49(6): p. 2129-2143.
- Wong, T., et al., 2018 Sydney Gay Asian Men Survey: Brief report on findings. 2018, Centre for Social Research in Health, UNSW: Sydney.
- Aung, E., Qualitative interviews with overseas-born MSM from non-English speaking countries, recently diagnosed with HIV, in CALD Gay Men’s Action Group Sympostium. 2019: Sydney.
- Circa, Research into community attitudes towards Pre-Exposure Prophylaxis. 2019, Australian Federation of AIDS Organisations: Sydney.
- Ensor, S., et al., The effectiveness of demand creation interventions for voluntary male medical circumcision for HIV prevention in sub-Saharan Africa: a mixed methods systematic review. Journal of the International AIDS Society, 2019. 22 Suppl 4(Suppl Suppl 4): p. e25299-e25299.
- Schaefer, R., et al., HIV prevention cascades: a unifying framework to replicate the successes of treatment cascades. The Lancet HIV, 2019. 6(1): p. e60-e66.
- Bass, E., et al., Demand creation for primary biomedical prevention: identifying lessons across interventions to inform daily oral preexposure prophylaxis programs. Curr Opin HIV AIDS, 2019. 14(1): p. 28-40.
- Holt, M., et al., Willingness to use HIV pre-exposure prophylaxis and the likelihood of decreased condom use are both associated with unprotected anal intercourse and the perceived likelihood of becoming HIV positive among Australian gay and bisexual men. Sex Transm Infect, 2012. 88(4): p. 258-63.
- Golub, S.A. and J.E. Myers, Next-Wave HIV Pre-Exposure Prophylaxis Implementation for Gay and Bisexual Men. AIDS Patient Care and STDs, 2019. 33(6): p. 253-261.
- Holt, M., et al., Increasing preexposure prophylaxis use and ‘net prevention coverage’ in behavioural surveillance of Australian gay and bisexual men. AIDS, 2021. 35(5).
- ACON. New ways to take PrEP. 2021 [cited 2021 June 30]; Available from: https://endinghiv.org.au/blog/new-ways-to-take-prep/.
- Wells, W., Biomedical HIV prevention, sexual pleasure and intimacy, in Australasian HIV & AIDS Cnference. 2019: Perth.
- Keen, P., et al., Use of HIV Pre-exposure Prophylaxis (PrEP) Associated With Lower HIV Anxiety Among Gay and Bisexual Men in Australia Who Are at High Risk of HIV Infection: Results From the Flux Study. J Acquir Immune Defic Syndr, 2020. 83(2): p. 119-125.
- Cambiano, V., et al., Cost-effectiveness of pre-exposure prophylaxis for HIV prevention in men who have sex with men in the UK: a modelling study and health economic evaluation. The Lancet Infectious Diseases, 2018. 18(1): p. 85-94.
- Nichols, B.E., et al., Cost-effectiveness analysis of pre-exposure prophylaxis for HIV-1 prevention in the Netherlands: a mathematical modelling study. The Lancet Infectious Diseases, 2016. 16(12): p. 1423-1429.
- Brewer, N.T., et al., Increasing Vaccination: Putting Psychological Science Into Action. Psychol Sci Public Interest, 2017. 18(3): p. 149-207.
Acknowledgements
Many thanks to the informants who I interviewed and/or discussed ideas with for this essay. I am also very grateful to both Associate Professor Edwina Wright and Professor Martin Holt for undertaking a technical review of the content. Thanks also to Dr Jeanne Ellard who commissioned, managed, and edited the essay.
Author details
Dean Murphy has worked at three national research centres (which contribute to Australia’s national strategies on drugs/alcohol, HIV, viral hepatitis, and sexually transmissible infections). He has also undertaken research at the Department of Gender and Cultural Studies, University of Sydney, and in the Department of Infectious Diseases, Alfred Hospital. His work focuses on biomedical HIV prevention technologies, stigma, HIV diagnosis, experiences of sexual health and well-being, and the meanings of drug consumption. His book, Gay Men Pursuing Parenthood Through Surrogacy: Reconfiguring Kinship, was published in 2015. He previously worked at the Australian Federation of AIDS Organisations where he developed HIV prevention campaigns. His current research projects include: acceptability of COVID-19 vaccines among Australian populations; changes in sexual practices, drug consumption, and health-seeking behaviour during the COVID-19 pandemic; and experiences of sexual health among young Aboriginal people.