
Decriminalisation of sex work: the evidence is in
Decriminalisation of sex work: the evidence is in
HIV Australia | Vol. 13 No. 1 | March 2015
By Jules Kim, Scarlet Alliance, Australian Sex Workers Association
Sex workers have been advocating for decades for the full decriminalisation of sex work and now it seems we have very persuasive evidence from The Lancet series on HIV and sex workers.1
Launched at AIDS 2014, the series examined the enablers and barriers to preventing and treating HIV infection in high, middle and low income countries with varying rates of HIV among sex workers.
The findings were consistent across all settings. Researchers found that the ‘decriminalisation of sex work would have the greatest effect on the course of HIV epidemics across all settings, averting 33–46% of HIV infections in the next decade’.2
The evidence clearly suggests that in order for biomedical prevention approaches to be successful, removal of structural barriers – including law reform and addressing stigma – remain critical.
Without the support of enabling environments, through the full decriminalisation of sex work, barriers will remain far too substantial for biomedical prevention alone to succeed.
The Lancet makes the important distinction between decriminalisation of sex work and what is often referred to as the legalisation (or licensing) of sex work.3
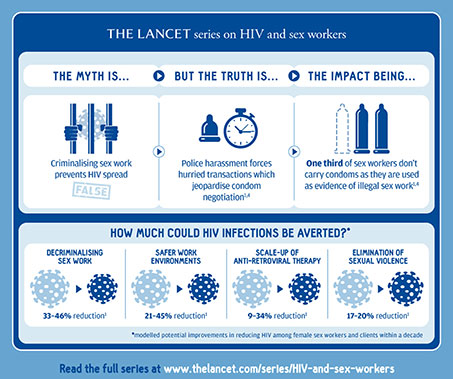
Figure 1: Excerpt from an infographic drawn from The Lancet series on HIV and sex workers.4
Decriminalisation of sex work applies to laws that criminalise consensual sex and related activities, including laws criminalising sex work; buying, soliciting, or procuring; brothel-keeping and management of sex work; and vagrancy, loitering, and public nuisance that are also used to target sex workers or clients.
In some countries it also applies to laws that criminalise same-sex consensual sex and laws that criminalise what is termed as ‘the impersonation of another sex’.5
The objective of legalisation is containment and control (and often surveillance) of sex work/ers, whereas the objective of decriminalisation is to uphold human rights and the occupational health and safety of sex workers.
Under decriminalisation criminal laws still apply to sex work, as they would to any other person or business. However, decriminalisation means that sex work is no longer seen as a crime but as work, and therefore, is subject to industrial regulatory mechanisms.
In the Australian context under a decriminalised system, sex industry businesses are treated like any other business.
They are subject to existing regulatory mechanisms, such as: local council planning; zoning controls; workers compensation requirements; occupational health and safety standards; and industrial rights obligations.
Decriminalisation does not mean no regulation. Decriminalisation means whole of government regulation. Importantly, police are not involved as regulators at any level unless there is a breach of law.
Decriminalisation supports the development and enforcement of occupational health and safety standards, access to industrial rights protections, and allows sex workers to organise for better working conditions.
Researchers Shannon, Strathdee, et al., conducted a systematic review of available epidemiological data on HIV and female sex work.6
They reviewed the role of structural determinants, i.e. contextual factors that reduce or increase the potential of HIV risk in HIV epidemics among female sex workers.
They reviewed 3,214 relevant studies published in the last six years (2008–2013) on HIV (or HIV/STI) prevalence/ incidence or condom use outcomes in relation to female sex work.
The researchers found that: ‘macro-structural factors increasingly play a central role in HIV epidemic structures among female sex workers’ operating in recurring pathways with other structural, behavioural and biological factors.7
‘Our review and modelling emphasise that macro-structural changes (eg, decriminalisation of sex work; and addressing of migration and stigma), and work environment features (eg, reductions or elimination of violence, police harassment, and implementation of supportive venue-based policies and practices) that they engender, are crucial to stem HIV epidemics in sex workers and clients,’ the researchers said.8
To assess the population-level impact of key structural drivers, ‘deterministic transmission dynamic models’ were used by the researchers to simulate the course of HIV epidemics and potential HIV infections averted through structural changes in female sex work in three settings (encompassing high, middle and low income countries and differing rates of HIV).9
The research modelled potential improvements in reducing HIV within a decade through: the elimination of violence, safer work environments, sex worker organising and improved ART coverage.
Results of the meta-analysis determined that, ‘decriminalisation of sex work could have the largest impact on the course of HIV epidemics across all three settings, averting 33–46% of incident HIV infections over next decade among female sex workers and clients’.10
In South India, the researchers observed that behavioural HIV prevention efforts such as peer-led outreach, sex worker collectivisation, drop-in spaces, access to clinics and sex worker advocacy to local government, as well as structural and sex worker-led efforts on policy, police and stakeholder engagement and training, had already resulted in substantial impact on both macro-structural and work environment determinants of HIV, thus the research modelling showed only modest impact from further sex worker empowerment-centred responses (grouped in Figure 2 as ‘SW collectivization’).11
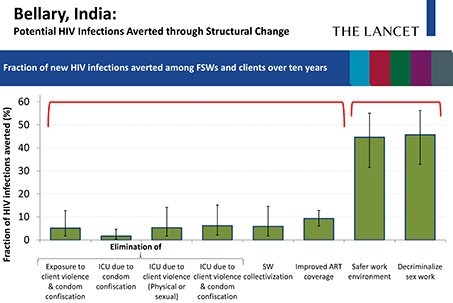
Figure 2: Bellary, India – potential HIV infections averted through structural change.17
Likewise, structural and sex worker led efforts had already resulted in large scale reductions in violence, thus the research modelling showed that elimination of physical violence and cessation of condom confiscation by police would only result in a further 6% reduction of HIV over the next decade; however, decriminalisation of sex work would avert up to 46% of HIV infections among female sex workers and clients over the next decade through its immediate and sustained effect on violence, policing, safer work environments, and condom use.12
As in other settings, researchers observed that scale and reach would only be feasible alongside legislative reform.
In Canada (Figure 3), the researchers found access to safer work environments could avert 34% of HIV infections among female sex workers and clients – but they also found that this would only be feasible alongside legislative reform.
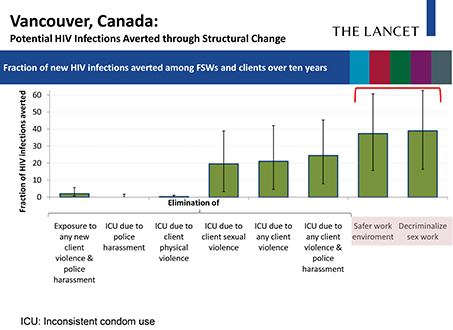
Figure 3: Vancouver, Canada – potential HIV infections averted through structural change.18
However, decriminalisation of sex work, through immediate and sustained impacts on violence, police harassment and safer work environments, and condom use could avert 39% of HIV infections among female sex workers and clients over the next decade.13
The researchers note that the potential impact of decriminalising sex work on rates of HIV could be further enhanced by the increased access to HIV prevention and treatment.
The percentages posited in the modeling of the impact of decriminalisation do not take this likely increased impact into account.14
The findings confirm the need for law reform and community-led interventions, to reduce HIV and promote human rights for sex workers globally. There has been a lot of emphasis on biomedical interventions and calls for population level antiretroviral treatment (ART) to end HIV.
The World Health Organization’s guidelines recommend a scale-up of ART to end the HIV epidemic.
However the research has found that scale-up of ART alone will avert HIV infection by 9–34% in contrast to the 33–46% reduction achieved by decriminalising sex work alone.15
This research demonstrates that to be effective ART must occur in tandem with structural change and sex worker-led efforts. In order to achieve an effective HIV response, there is a critical need for structural change, (i.e., decriminalisation of sex work, elimination of violence, police harassment, safer work environments).
The Lancet and other research supports that decriminalising sex work would also have immediate impacts on eliminating violence, police harassment and creating safer work environments.
Over 100 sex workers from 30 countries attending the AIDS 2014 Sex Worker Pre-conference agree.
This is clearly articulated in the sex worker consensus statement on biomedical developments: ‘Current and existing implementations of biomedical approaches are doomed to fail because they don’t take into account discriminatory legal frame works that create barriers for sex workers.
Legal barriers for sex workers are still so significant that unless we resolve those issues first, through the full decriminalisation of sex work, test and treat or treatment as prevention are abstract concepts that have no meaning for sex workers but will divert resources away from approaches that we know work’.16
In fact, one of the main outcomes from the AIDS 2014 conference was the unanimous, united call for decriminalisation of sex work. Encouragingly, AIDS 2014 saw members of parliament from the region committing to rights-based reform to tackle HIV/AIDS in their countries.
Papua New Guinean Health Minister, Michael Malabag, committed to introducing legislation to decriminalise sex work as a key reform to tackling HIV in his nation. Other MPs from the Asia-Pacific region, such as Fiji, Nepal and Indonesia also committed to dialogue with sex workers.
‘I will bring in the legislation. We must remove the stigma. We are all equal,’ Papua New Guinea Health Minister Malabag told the audience of civil society representatives, academics, parliamentarians and activists at AIDS 2014.19
Nepal MP Rajeev Shah told the audience that: ‘We are Members of Parliament but we don’t know everything. MPs must listen and work with civil society to bring about rights-based changes to end HIV/AIDS’.20
In their Lancet series article, An action agenda on sex workers and HIV,
Professor Chris Beyrer (Professor of Epidemiology, International Health, and Health, Behaviour, and Society at the Johns Hopkins University Bloomberg School of Public Health and President of the International AIDS Society) and Michel Sidibé (UNAIDS Executive Director) along with a number of experts, including sex worker Anna-Louise Craigo, are united in their call for decriminalisation of sex work:
‘Legal environments, policies and police practices continue to challenge sex workers’ abilities to protect themselves, their families, and their sexual partners from HIV … To address HIV in sex workers will need structural and policy reform’.21
They are clear in the manifold impact of decriminalisation on HIV prevention, treatment and support as well as the substantial cost savings that would be achieved if sex work was decriminalised.
They also outline other potential benefits and cost savings that would result from the decriminalisation of sex work.
‘In addition to HIV prevention, other societal benefits could include raised access to police protection, improved occupational health and safety in sex work, and the redirection of law enforcement and criminal justice expenditures towards health and social services’.22
They call on governments to, ‘Decriminalise sex work, decriminalisation can improve the risk environment. Advance evidence-based policies, and practices in partnership with sex worker-led organisations’.23
The Lancet clearly demonstrates the evidence of the need for and the many benefits of decriminalisation.
Sex workers and sex worker activists have been calling for decriminalisation for many years for our rights, health and safety. The evidence from NSW, where sex work was decriminalised in 1995, has been compelling and held up worldwide as an example.
The UNAIDS, UNFPA and UNDP report Sex Work and the Law in the Asia Pacific states:
‘Evidence from the jurisdictions in the region that have decriminalized sex work (New Zealand and New South Wales) indicates that the approach of defining sex work as legitimate labour empowers sex workers, increases their access to HIV and sexual health services and is associated with very high condom use rates’.24
The ‘positive public health and human rights outcomes’ achieved in NSW are well documented,25, 26, 27, 28 yet sex workers in NSW still have to fight to maintain decriminalisation.
Globally and within the region, there has been a noticeable shift towards the recognition of the essential need for the decriminalisation of sex work.
It is vital to effectively addressing HIV and a number of influential supporters, including politicians, policy makers and international bodies have spoken publically in support of decriminalisation of sex work.
There is an urgent need for action as Australia risks falling behind, where we have previously led the way.
There is irrefutable support and evidence for decriminalisation of sex work, our workplaces and our clients.
In order to achieve this now, sex workers require the support from stakeholders in the HIV response and leadership from government and policy makers, in advocating for what is necessary to advancing HIV prevention, treatment and care in Australia.
For further information on The Lancet series on HIV and sex workers, see Scarlet Alliance’s summary available at: bit.ly/1MSGOKh
References
1 The Lancet. (2015). HIV and sex workers series [online]. Available at: www.thelancet.com
2 Shannon, K., Strathdee, S., Goldenberg, S., Duff, P. , Mwangi, P., Rusakova, M., et al. (2015). Global epidemiology of HIV among female sex workers: influence of structural determinants. The Lancet, 385(9962), 55–71. dx.doi.org/10.1016/S0140-6736(14)60931-4
3 Decker, M., Crago, A., Chu, S., Sherman, S., Seshu, M., Buthelezi, K., et al. (2015). Human rights violations against sex workers: burden and effect on HIV. The Lancet, 385(9963), 186–199. dx.doi.org/10.1016/S0140-6736(14)60800-X
4 The full infographic from The Lancet series on HIV and sex work is available at: http://www.thelancet.com/pb/assets/raw/Lancet/stories/commissions/Lancet-sex-work-infographic_fullsize.pdf
5 Poteat, T., Wirtz, A., Radix, A., Borquez, A., Silva-Santisteban, A. Deutsch, M., et al. (2015). HIV risk and preventive interventions in transgender women sex workers. The Lancet, 385 [Online], 274–286. dx.doi.org/10.1016/S0140-6736(14)60833-3
6 Shannon, K., et al. (2015). op. cit.
7 Strathdee, S., et al. (2015, 22 July). The Global Epidemiology of HIV among Female Sex Workers: The Influence of Structural Determinants. Paper presented at the 20th International AIDS Conference, Melbourne, abstract TUSY0402. Retrieved from: pag.aids2014.org
8 Beyrer, C., Crago, A., Bekker, L., Butler, J., Shannon, K., Kerrigan, D., et al. (2014). An action agenda for HIV and sex workers. The Lancet, 385(9964), 287–301. dx.doi.org/10.1016/S0140-6736(14)60933-8
9 Shannon, K., et al. (2015). op. cit.
10 Strathdee, S., et al. (2015, 22 July). op. cit.
11 ibid.
12 ibid.
13 ibid.
14 Shannon, K., et al. (2015). op. cit.
15 ibid.
16 Sex Worker Pre-conference AIDS 2014 Consensus Statement. Retrieved from: www.scarletalliance.org.au
17 Strathdee, S., et al. (2015, 22 July). op. cit.
18 Strathdee, S., et al. (2015, 22 July). op. cit.
19 18 Live coverage of AIDS 2014. Crowd 360.org. Retrieved from: crowd360.org
20 ibid.
21 Beyrer, C., Crago, A., Bekker, L., Butler, J., Shannon, K., Kerrigan, D., et al. (2015). op. cit.
22 ibid.
23 ibid.
24 Godwin, J. (2012). Sex Work and the Law in the Asia Pacific. Laws, HIV and human rights in the context of sex work. United Nations Development Program (UNPD) Asia-Pacific Regional Centre, Bangkok. 6 Retrieved from: www.undp.org
25 ibid.
26 Donovan, B., Harcourt, C., Egger, S., Watchirs Smith, L., Schneider, K., Kaldor, et al. (2012). The Sex Industry in New South Wales: a Report to the NSW Ministry of Health. The Kirby Institute, University of New South Wales, Sydney.
27 New South Wales Government. (2001). Report of the Brothels Task Force. New South Wales Government.
28 Harcourt, C., O’Connor, J., Egger, S., Fairley, C., Wand, H., Chen, M., et al. (2010). The decriminalisation of prostitution is associated with better coverage of health promotion programs for sex workers. Aust NZ J Public Health, 34, 482–486. dx.doi.org/10.1111/j.1753-6405.2010.00594.x